


How to Differentiate Rheumatism from Rheumatoid Arthritis

Rheumatism and rheumatoid arthritis are two common conditions managed by rheumatology and immunology departments. Most patients present with joint-related symptoms, which can easily lead to misdiagnosis. Careful differential diagnosis is essential to avoid delays in appropriate treatment. So, how can one distinguish between rheumatism and rheumatoid arthritis?
How to Differentiate Rheumatism from Rheumatoid Arthritis
Differentiating rheumatism from rheumatoid arthritis requires careful evaluation of specific clinical features. Rheumatism (i.e., rheumatic fever–related arthritis) commonly affects adolescents and typically manifests as monoarticular arthritis—most frequently involving large joints such as the knees and elbows. Laboratory findings usually show elevated inflammatory markers, including antistreptolysin O (ASO), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP); antinuclear antibody (ANA) testing is generally negative. Treatment is primarily symptomatic, using anti-inflammatory and analgesic medications. In contrast, rheumatoid arthritis predominantly occurs in middle-aged and older women. Its classic presentation includes bilateral, symmetric swelling and pain in small joints. Morning stiffness is a hallmark symptom, gradually improving with appropriate joint movement. Laboratory tests typically reveal positivity for rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies; inflammatory markers may also be significantly elevated.
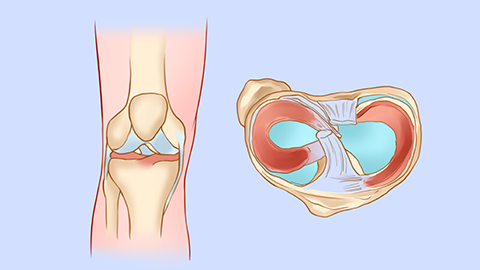
Generally speaking, “rheumatism” refers to arthritis secondary to rheumatic fever—a condition distinct from rheumatoid arthritis. Regarding joint involvement, rheumatic arthritis primarily affects large joints—such as the knees, elbows, and shoulders—and tends to be asymmetric. It is characterized by migratory, highly active inflammation that may rapidly shift from one joint to another. Importantly, joint deformities and bony destruction rarely occur following resolution of inflammation. By contrast, rheumatoid arthritis typically involves small joints of the extremities—including the fingers, toes, wrists, and ankles—usually in a symmetric pattern and accompanied by morning stiffness.
Therefore, when joint pain occurs in various parts of the body, it may indicate either rheumatism or rheumatoid arthritis—distinguishing between them relies on the above clinical and laboratory features. We hope this explanation proves helpful.