


How is cervical grade 3 lesion treated?
I haven’t had a gynecological examination since giving birth to my baby. Recently, I’ve experienced some vaginal discomfort, so my husband accompanied me to the hospital for an evaluation—and I was diagnosed with cervical grade III lesion. How is cervical grade III lesion treated?
How is cervical grade III lesion treated?
Once confirmed pathologically as a cervical grade III lesion, clinical guidelines recommend cervical conization (cone biopsy). Avoid sexual intercourse for 3–7 days after menstruation ends. Prior to surgery, it’s advisable to ensure normal vaginal discharge (i.e., no active infection), and complete preoperative blood tests—including coagulation profile and electrocardiogram (ECG). If all test results are normal, cervical conization is recommended. Cervical grade III lesion is essentially a precancerous condition and must be taken seriously in clinical practice. Even after conization, the excised tissue must be sent for pathological examination to confirm whether the entire lesion has been completely removed.
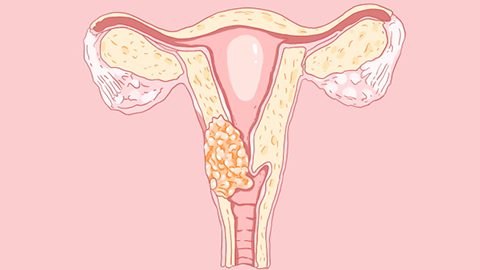
If residual lesion remains after surgery, repeat surgery may be necessary. If the lesion is completely excised, follow-up screening with liquid-based cytology (TCT) and human papillomavirus (HPV) testing every six months is recommended to monitor for local cervical abnormalities or persistent high-risk HPV infection. Cervical grade III lesion is clinically referred to as “cervical precancerous lesion” or “cervical intraepithelial neoplasia (CIN),” and cervical lesions are classified into three grades—CIN I, CIN II, and CIN III—based on severity.
Cervical grade III lesion represents the most advanced stage of cervical precancerous disease. Without prompt and appropriate treatment, it may progress to invasive cervical cancer—a potentially life-threatening condition. We hope this information is helpful to you!