


What is mammary duct ectasia?
Benign breast hyperplasia and breast cancer are relatively common conditions among women and can significantly impair normal postpartum lactation. If mammary duct ectasia is not promptly diagnosed and treated, it may lead to breast distortion or deformity. So, what exactly is mammary duct ectasia?
What Is Mammary Duct Ectasia?
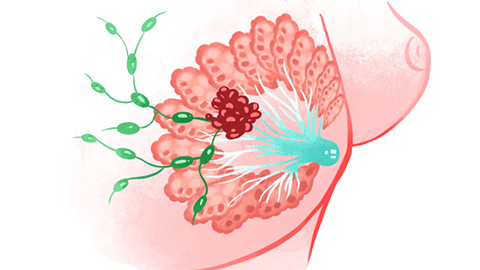
Plasma cell mastitis—also known as plasma cell mastitis (PCM), ductal mastitis, or duct ectasia syndrome—and referred to in Traditional Chinese Medicine (TCM) as “acne-like mastitis,” is the most common non-bacterial inflammatory condition occurring in non-lactating women. Its exact etiology remains unclear. The condition predominantly affects middle-aged and elderly individuals and may result from nipple inversion or malformation, or from squamous epithelial cells migrating into the ductal lumen, causing keratinized desquamation and subsequent ductal obstruction. Accumulated lipid secretions then irritate the ductal wall, triggering inflammation, fibrotic scarring, and secondary infection—ultimately leading to degenerative changes.
It may also represent an autoimmune disorder; in later stages, it frequently co-occurs with plasma cell mastitis. Histopathologically, the hallmark is extensive infiltration by plasma cells. The disease tends to follow a relapsing-remitting course, and some clinicians classify it as an autoimmune condition.

Lesions typically involve only one breast, although bilateral involvement may occur. Nipple discharge may be the initial and sole presenting sign. Gentle compression at multiple sites around the breast often elicits discharge from the nipple. The disease commonly affects numerous lactiferous ducts and may extend across much of the areolar region. Nipple discharge is usually intermittent—appearing and disappearing unpredictably.