


Treatment Options for Adenomyoma
Uterine adenomyoma significantly impacts the daily lives of many patients and requires timely treatment. What are the treatment options for uterine adenomyoma?
Treatment Options for Uterine Adenomyoma
The choice of treatment for uterine adenomyoma should be individualized based on symptom severity, patient age, and fertility requirements. For patients with mild symptoms, those desiring future fertility, or those approaching menopause, medical therapy—such as gestrinone or gonadotropin-releasing hormone agonists (GnRHa)—can effectively alleviate symptoms. Younger patients or those wishing to preserve fertility may consider focal excision (adenomyoma resection). In contrast, patients with severe symptoms, no desire for future childbearing, and inadequate response to medical therapy typically require total hysterectomy. Whether to preserve the ovaries depends on the presence of ovarian pathology and the patient’s age. Additionally, laparoscopic presacral or sacral nerve ablation may be considered for refractory dysmenorrhea.
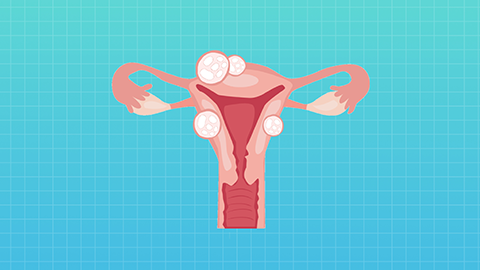
Uterine adenomyoma refers to the ectopic presence of endometrial tissue within the myometrium—rather than within the uterine cavity—where it undergoes cyclical shedding in synchrony with the menstrual cycle. However, because this ectopic tissue cannot be expelled, it bleeds into the myometrium. The resulting blood is gradually absorbed by the body, triggering reactive fibrosis, tissue proliferation, and adhesion formation—ultimately leading to adenomyoma development. Patients commonly experience menorrhagia and prolonged menstrual periods. On gynecological examination and ultrasound, the uterus typically appears diffusely and uniformly enlarged, often with a spherical contour—helping differentiate adenomyoma from leiomyoma (fibroids).
In a minority of cases, adenomyosis manifests as localized nodules or masses—termed “adenomyomas”—which arise from repeated hemorrhage within the myometrium. This leads to surrounding fibrous tissue proliferation, resulting in ill-defined margins between the lesion and adjacent myometrium, making surgical excision technically challenging. We hope this information proves helpful to you!